by Evelyn Adkins
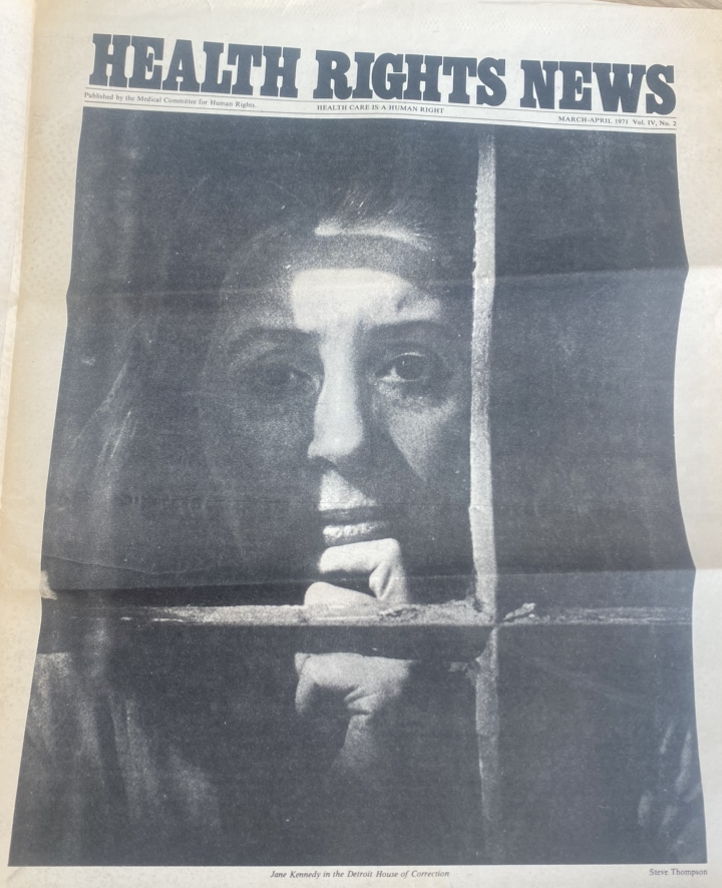
Newspaper clipping from Health Rights News1
Discussing how male supremacy in the medical industry has historically affected women’s access to healthcare. As well as analyzing how these past decisions affected women’s access to healthcare today by examining the complex intersections of healthcare, inequality, and social justice.
Doctor Knows Best? Transcript
Hello everyone welcome to today’s podcast episode, Doctor Knows Best, where we will examine the complex intersections of healthcare, inequality, and social justice. I’m your host, Evelyn, and today we’re diving into a system that was created by men but relied on by women.
The healthcare system has historically been rooted in patriarchal values and institutionalized practices that oppress women. Furthermore, women have historically been underrepresented and misunderstood in the medical community. Today I want to look back and ask how has male supremacy in the medical industry historically affected women’s access to healthcare. As well as, how do these past decisions and structures affect women’s access to healthcare today?
Before we dive in, let me remind you that healthcare isn’t just about medical procedures; it’s about who has the power to shape the narratives and policies, as well as decide who gets access to care.
When we take a deeper look into the healthcare system, we see that women rely more on health services compared to men. The CDC reports that on average women are 33% more likely to visit the doctor than men2. Not only do women rely on general health care needed by an adult, they also need specialized services related to their reproductive system. We can also see that historically as mothers, women have also been responsible for their children’s doctor visits and overall healthcare3. Additionally, to build on this, 78% of the US healthcare workforce are women. Even though the majority of people working and relying on healthcare are women, it is still the male – doctors, deans, directors, trustees, and insurance companies – who make the decisions regarding female health. Historically this has led to men deciding women’s access and options to abortions, birth control, method of childbirth, and the crucial procedures that can make the difference between life and death.4 Due to the patriarchal structures of the healthcare industry, today we see a system created for men made by men, that excludes the millions of women who rely on the industry every day.
Furthermore when looking at which demographic has been the most underrepresented and exploited by the healthcare system is black women. After the importation of enslaved people from overseas was outlawed in 1808, slave owners had a new focus on their existing enslaved populations’ reproductive viability5. Additionally, medical experiments were performed on enslaved women. For example, Dr. J Marion Sims who was praised as the “father of modern gynecology”,6 developed new surgical techniques through experiments on enslaved women5. Medical experiments were often conducted without anesthesia due to the belief that black people felt less pain than white people.5 This racially biased perception regarding pain tolerance persists even today in modern medicine affecting how doctors view and treat pain among different racial groups5.
We need female and POC representation in these higher-up positions that make the crucial decisions on female reproductive health. However, throughout time women have been discouraged from entering these higher-up medical positions such as doctors, surgeons, or physicians because they are deemed as more masculine occupations.4 This has led to women being encouraged to enter more feminine health positions such as nurses.4 The enforcement of gender roles in occupations has led to the discrimination of women seeking higher-paying and more responsible positions in healthcare. It is these confinements to gender that have created a system that uplifts men and contains women.
One of the most essential resources for women to have bodily autonomy and planned parenthood is birth control. Access to contraceptives is crucial, especially in today’s day and age where reproductive rights are being taken away. Forms of contraceptives have existed for centuries. As early as 1850 BC ancient Egypt recorded the use of making mixtures to be rubbed on, swallowed, or inserted to prevent pregnancy were used.3 In the early 19th century, discussions emerged in Europe regarding the concern for the social and economic justifications for contraceptives.3 An English economist named Robert Thomas Malthus began predicting that a large population increase would cause poverty. Malthus’s philosophy is one of the major influences for the birth control movements in Europe and the US.3 In the US, birth control was deemed to have “four banners” that it could be advertised under including helping with, population control, “welfare syndrome”, the health of women, and finally the individual right of each woman to birth control. Birth control is crucial for women, both as a fundamental right and a matter of health. However, the focus of institutions who control and produce contraceptives in the U.S. is less about women’s health and more on issues like population control and “welfarism.” It is essential for women to recognize the underlying interests of the institutions providing these services.
A major example of this is in the 70s when birth control was in the early stages of being advertised throughout the US. The possible dangerous side effects of birth control were kept hidden from women.3 Any harmful side effects came under the heading of “classified” information.3 It took a woman named Barbara Seaman, who revealed the 50 possible side effects of contraception in her book The Doctors’ Case Against the Pill.3 Doctors and the FDA deliberately withheld crucial information about the medication they were attempting to “sell.” The side effects of birth control have the potential to be life-threatening, yet these male “experts” chose to remain silent.3 This reveals the extent of male bias in the medical field and its direct, harmful impact on women.3 As well as how these institutions will do anything to help their agenda even at the expense of women’s health
This new consciousness led me to dig deeper and ask more questions of how far this reality will go. I found an interesting concept that healthcare resources are being provided when they directly benefit the economy or government. This same theme can be seen in today’s social climate with US birth rates declining leading to the overturning of Roe v. Wade making abortions illegal and even criminalized. Additionally, with the development of the Project 2025 agenda wanting to further control women’s rights and bodily autonomy, the threat of banning contraceptives is becoming a possibility. This demonstrates that as soon as something doesn’t benefit the government or economy, they will take it away and women are already experiencing that reality today.
This pattern throughout the history of controlling women through medicine has great implications on the medical world today. For example, the Gender Equity Policy Institute said that in Texas, which has had some of the worst abortion restrictions in the country since 2019-2022 has seen a 56% increase in maternal mortality rate compared to the 11% increase nationwide.6 The increase in maternal mortality is only increasing with more bans and restrictions getting passed. Women are dying and the government is doing nothing to stop it. Male politicians are continuing to make laws that affect women’s access to healthcare, further uplifting the patriarchal values in the healthcare system today.
The time to fight is now. The history of patriarchy in healthcare is not just a relic of the past; but something continues to affect how women access and experience healthcare today. So I urge you to get involved, demand change, contact government officials donate to organizations that are fighting for our sister’s rights. Together we work toward a healthcare system that is more equitable, inclusive, and compassionate.
Thank you for tuning into Doctor Knows Best take care.
- Sophia Smith Collection of Women’s History, Abortion and Birth Control Committee: notes, forms, and correspondence, 1971 – 1972, Newspaper Clippings, Health Rights News ↩︎
- “Why Don’t Men See Doctors? | Integris Health.” Integris Health, integrishealth.org/resources/on-your-health/2019/june/why-dont-men-see-doctors. Accessed 27 Nov. 2024.
↩︎ - Sophia Smith Collection of Women’s History, Abortion and Birth Control Committee: notes, forms, and correspondence, 1971 – 1972, Health Policy Advisory Center, HEALTH PAC, Bulletin, No. 40, April 1972
↩︎ - Sophia Smith Collection of Women’s History, Abortion and Birth Control Committee: notes, forms, and correspondence, 1971 – 1972, Health Policy Advisory Center, HEALTH PAC, Bulletin, March 1970
↩︎ - “How History Has Shaped Racial and Ethnic Health Disparities: A Timeline of Policies and Events.” KFF, Medical Exploitation of Enslaved Black Women, 22 Oct. 2024, ↩︎
- Wailoo K. Historical Aspects of Race and Medicine: The Case of J. Marion Sims. JAMA. 2018;320(15):1529–1530. doi:10.1001/jama.2018.11944 ↩︎